We present summaries of select cases from our virtual tumor board: cases submitted by treating clinicians for ITMIG’s expert multidisciplinary opinion. The tumor board is composed of a moderator and at least one of the following specialists: thoracic surgeon, medical oncologist, radiation oncologist, diagnostic radiologist, and thoracic pathologist, all with significant interest and experience in thymic malignancies.
Virtual Tumor Board – cases
Submitted cases
Case presented in October 2021 at the 11th ITMIG Annual Meeting
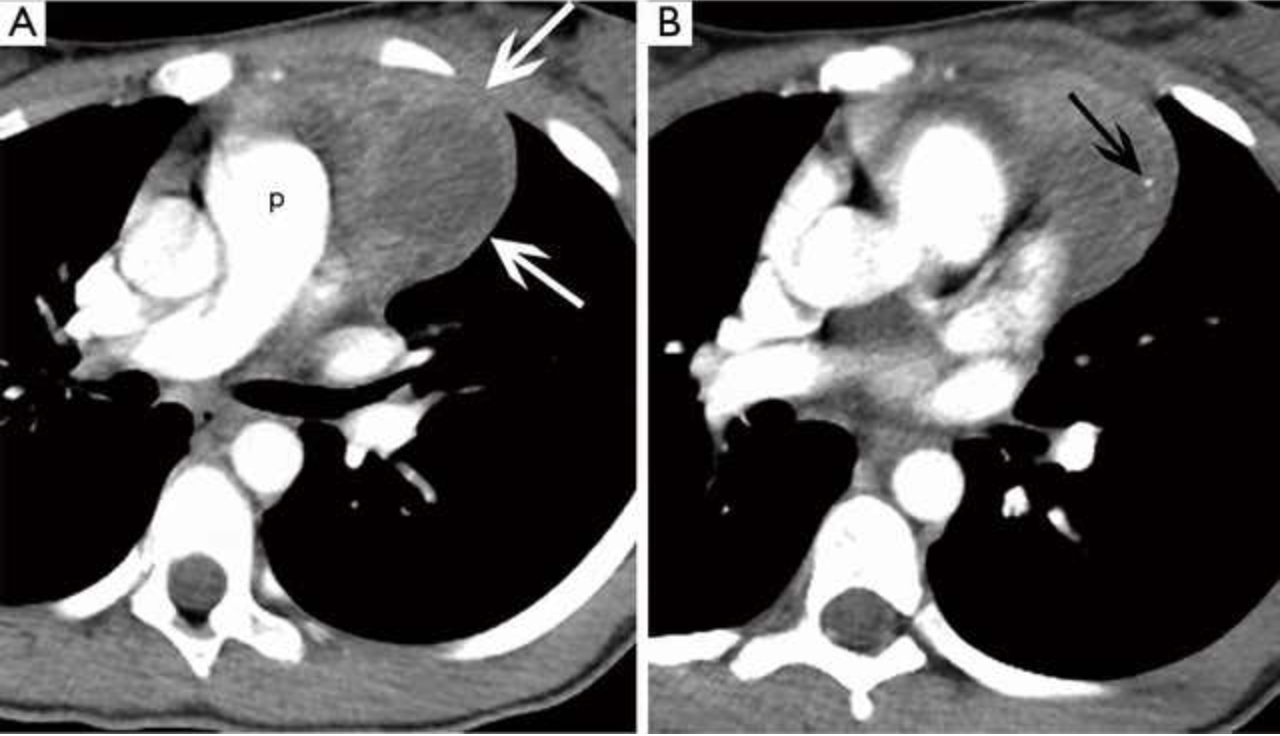
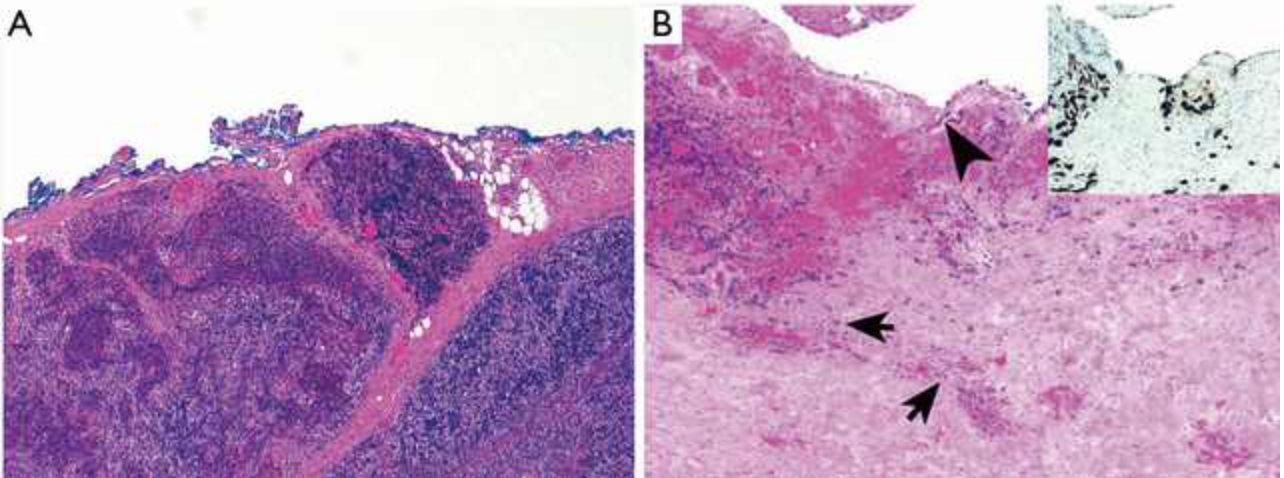
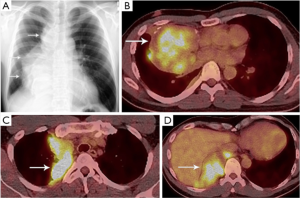 At the 11th International Thymic Malignancy Interest Group Annual Meeting, a multidisciplinary expert panel discussed the diagnosis and treatment strategies of a 37-year-old man with TNM IVA type B2B3 thymoma.
At the 11th International Thymic Malignancy Interest Group Annual Meeting, a multidisciplinary expert panel discussed the diagnosis and treatment strategies of a 37-year-old man with TNM IVA type B2B3 thymoma. 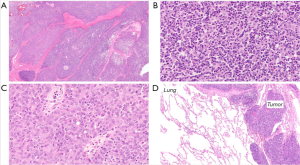
READ MORE…
Marcin Zielinski, Anja C. Roden, Mylene T. Truong, Dirk Van Raemdonck, Ritsuko Komaki, Heather Wakelee, Malgorzata Szolkowska, Mediastinum 2022;6:26
Case presented in April 2019
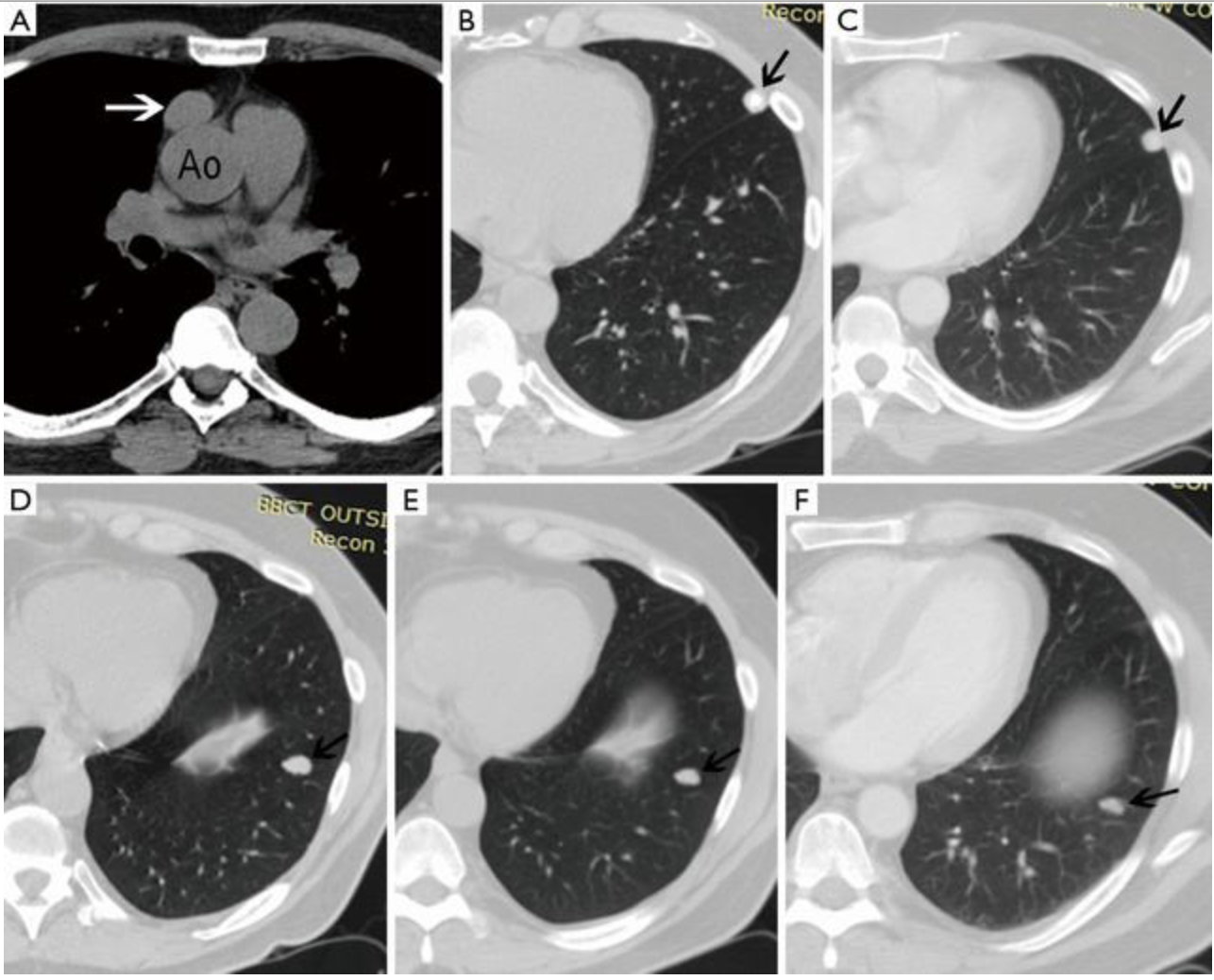
 A 58-year-old man with a 25-pack year smoking history was screened for lung cancer with a computed tomography (CT) scan of his chest. The only pertinent family history includes prostate carcinoma of the father and brother. The patient is otherwise healthy. An unenhanced chest CT demonstrates an ovoid 2.7×1.8 cm well-demarcated soft tissue mass in the prevascular mediastinum (Figure 1A), which is new compared to two prior chest CT scans performed 4 and 9 years prior.
A 58-year-old man with a 25-pack year smoking history was screened for lung cancer with a computed tomography (CT) scan of his chest. The only pertinent family history includes prostate carcinoma of the father and brother. The patient is otherwise healthy. An unenhanced chest CT demonstrates an ovoid 2.7×1.8 cm well-demarcated soft tissue mass in the prevascular mediastinum (Figure 1A), which is new compared to two prior chest CT scans performed 4 and 9 years prior.
READ MORE…
Sigurdson S, Roden AC, Marom EM, Szolkowska M, Girard N, Rajan A, Marino M, Rimnera A, Moideen N, Russell WE, Weksler B, Detterbeck FC, Falkson CB. Case presentation and recommendations from the April 2019 ITMIG tumor board: an international multidisciplinary team. Mediastinum 2019;3:41.
Case presented in April 2018
 An 11-year-old female who was previously healthy presented to her local Emergency Department with a one-week history of pain behind her left scapula and subjective low-grade fever. She had no respiratory or constitutional symptoms, no history of facial flushing, and an unremarkable physical exam. The patient’s past medical history includes a tonsillectomy more than 5 years prior following multiple febrile episodes, up to date immunizations, no medications, and there was no other contributing history. Her family history includes her mother being a BRCA1 carrier and diagnosed with breast cancer before the age of 50, a maternal cousin with juvenile rheumatoid arthritis, and her father is a hemoglobin C carrier.
An 11-year-old female who was previously healthy presented to her local Emergency Department with a one-week history of pain behind her left scapula and subjective low-grade fever. She had no respiratory or constitutional symptoms, no history of facial flushing, and an unremarkable physical exam. The patient’s past medical history includes a tonsillectomy more than 5 years prior following multiple febrile episodes, up to date immunizations, no medications, and there was no other contributing history. Her family history includes her mother being a BRCA1 carrier and diagnosed with breast cancer before the age of 50, a maternal cousin with juvenile rheumatoid arthritis, and her father is a hemoglobin C carrier.
 A chest radiograph obtained during her initial visit to the emergency department demonstrated a prevascular mediastinal mass. The patient was referred to the local pediatric hospital where she was admitted for additional work-up. To further investigate the mediastinal mass, a contrast-enhanced chest computed tomography (CT) was obtained.
A chest radiograph obtained during her initial visit to the emergency department demonstrated a prevascular mediastinal mass. The patient was referred to the local pediatric hospital where she was admitted for additional work-up. To further investigate the mediastinal mass, a contrast-enhanced chest computed tomography (CT) was obtained.
READ MORE…
Sigurdson SS, Roden AC, Marom EM, Detterbeck FC, Falkson CB. Case presentation and recommendations from the April 2018 ITMIG tumor board: an international multidisciplinary team. Mediastinum 2019;3:4.
Cases presented in October 2017
 CASE 1: A 72-year-old woman presented to the Emergency Department after a fall complaining of bilateral leg weakness. She had polio as a child, but no other contributing history. On physical examination her vital signs were normal as well as her neurological examination. She had normal reflexes, no neurological deficits, and no leg weakness.
CASE 1: A 72-year-old woman presented to the Emergency Department after a fall complaining of bilateral leg weakness. She had polio as a child, but no other contributing history. On physical examination her vital signs were normal as well as her neurological examination. She had normal reflexes, no neurological deficits, and no leg weakness.
As part of the routine investigation, a chest radiograph was obtained which demonstrated a prevascular mass abutting and inseparable from the right heart border (Figure 1A). To further investigate this mass, a contrast-enhanced chest CT scan (Figure 1B) was obtained followed by a chest MRI (Figure 1C,D). Upon review of the images the tumor board radiologist described the mass as a homogenous fluid density prevascular mass, most suggestive of a benign cyst.
READ MORE…
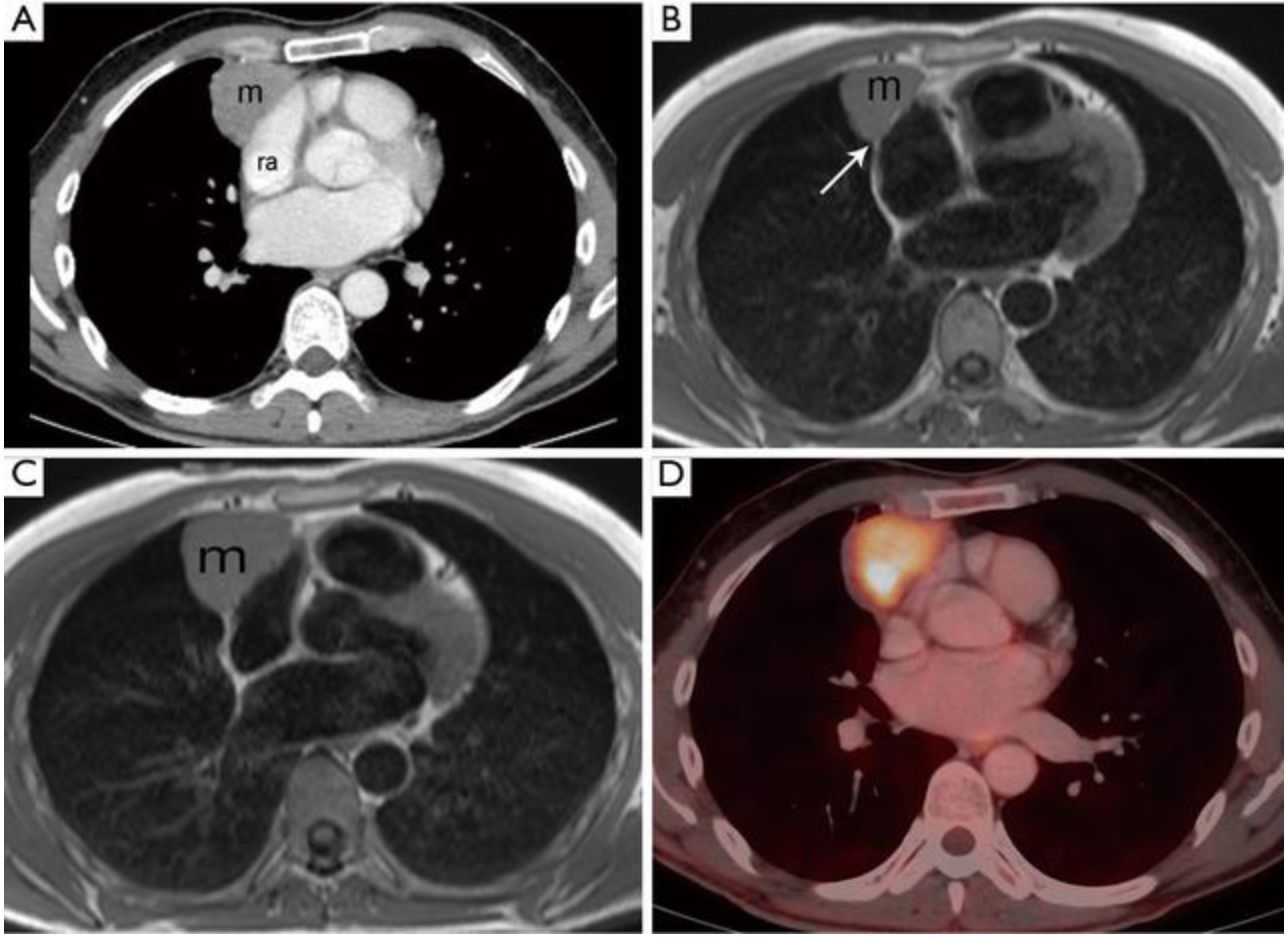 CASE 2. As part of his routine medical check-up, a 51-year-old asymptomatic marathon runner had a chest radiograph, which revealed a mediastinal mass. His physical examination was normal. Four years before that he had had pericarditis which was diagnosed by clinical symptomatology and echocardiography, presumed to be of viral etiology, and the patient recovered with non-steroidal anti-inflammatory medication.
CASE 2. As part of his routine medical check-up, a 51-year-old asymptomatic marathon runner had a chest radiograph, which revealed a mediastinal mass. His physical examination was normal. Four years before that he had had pericarditis which was diagnosed by clinical symptomatology and echocardiography, presumed to be of viral etiology, and the patient recovered with non-steroidal anti-inflammatory medication.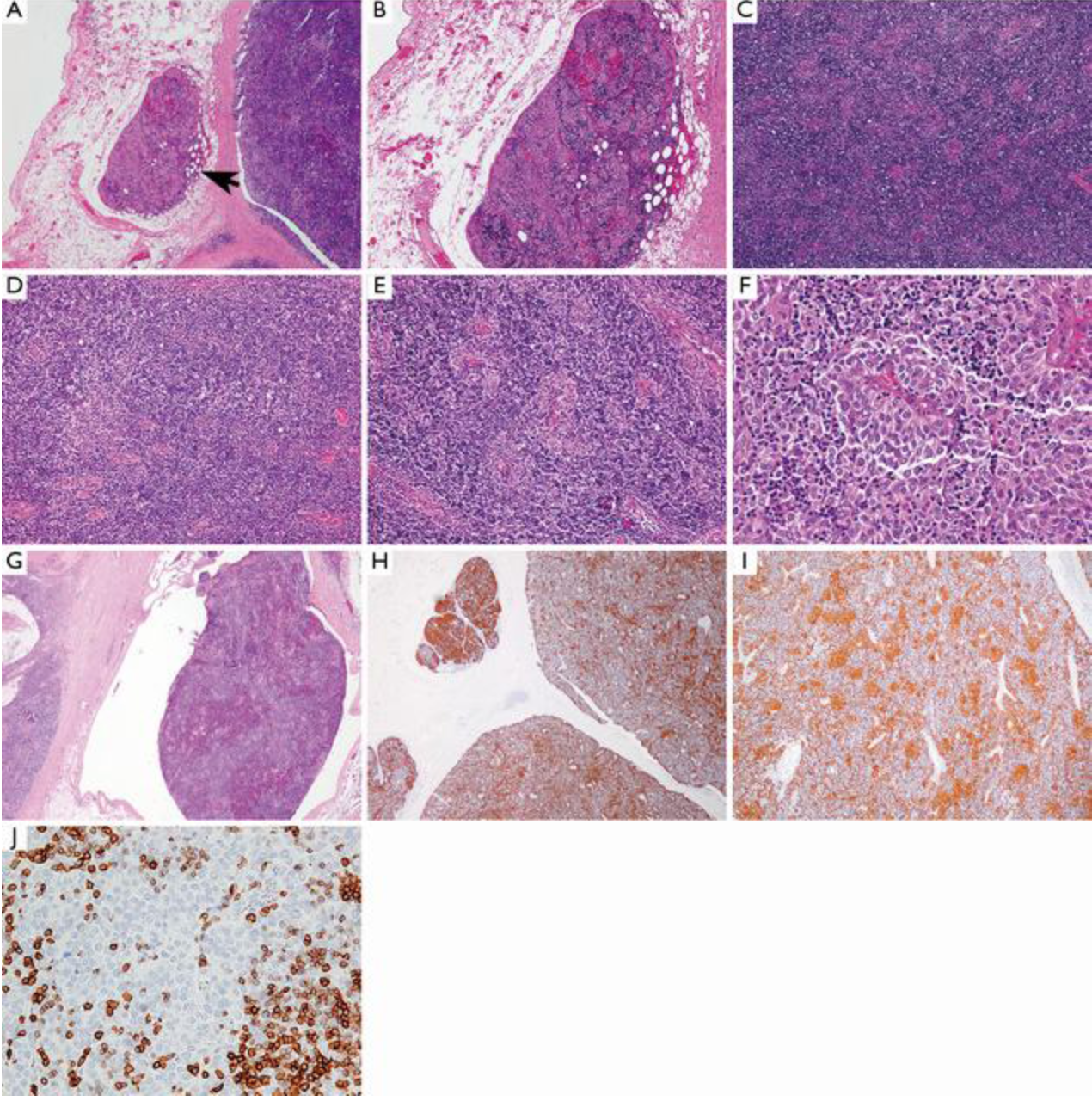
Following the chest radiograph, the patient had a chest CT, chest MRI, and whole body FDG PET-CT that were reviewed by the diagnostic radiologist on the tumor board. The chest CT demonstrates a prevascular soft tissue mass (Figure 2A) which abuts the right atrium.
READ MORE…
Sigurdson S, Marom EM, Roden AC, Detterbeck FC, Falkson CB. Case presentations and recommendations from the October 2017 ITMIG tumor board: an international multidisciplinary team. Mediastinum 2018;2:53.